The Maternal Health Crisis in Texas: Visibility, Access, and Systemic Failure
SEPTEMBER 2021
Texas has the highest rate of maternal mortality in the United States, while maternal mortality rates continue to decline across most other industrialized nations¹. Why?
I volunteered with a nonprofit organization supporting mothers in the greater Dallas area. Through that work, I began to understand more deeply how healthcare policy, economic inequality, and access to reproductive care intersect to shape maternal health outcomes.
What began as research into maternal mortality evolved into a broader examination of how systems fail, and how design influences whether those failures are visible or ignored. The most obvious takeaway is that there are substantial gaps in accessibility to maternal care. Despite spending more per capita on healthcare than any other country, maternal health outcomes in the United States remain significantly worse than those of comparable nations¹.
A challenge I faced while researching this issue was not finding statistics, it was understanding how to communicate the scale of the crisis in a way that felt legible, human, and impossible to dismiss. Since data alone rarely creates urgency, I focused on clear context, narrative structure, and visual communication to shape how systemic issues could actually be understood.
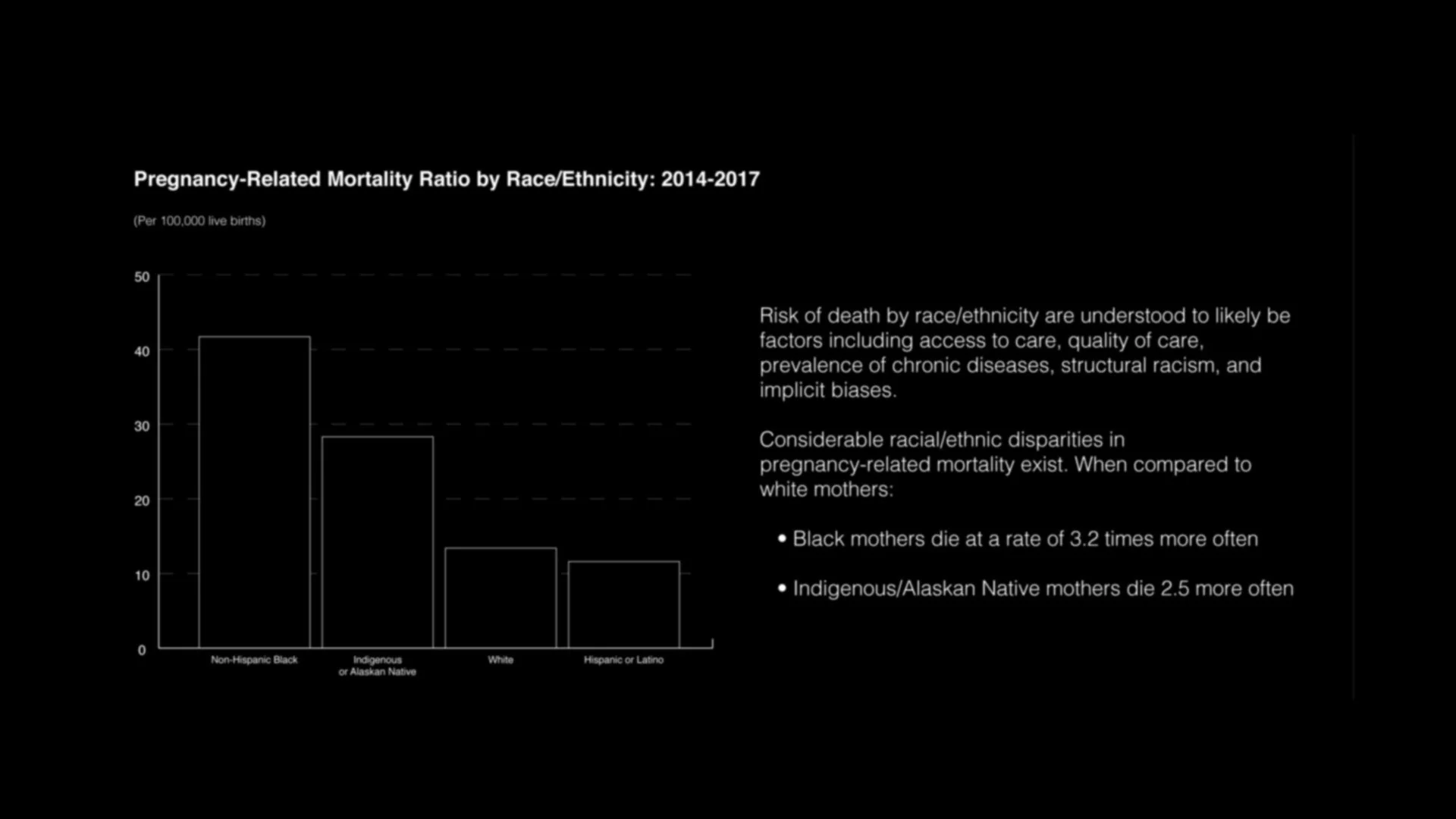
Maternal mortality reflects a broader overlap of systemic discrimination, economic inequality, and gaps in access to affordable healthcare. In many communities, particularly those already facing structural disadvantage, equitable maternal care remains difficult to access.
In Texas, access to reproductive healthcare has become increasingly restricted. As of September 1, 2021, abortion became illegal once fetal cardiac activity can be detected, often around six weeks of pregnancy². Introduction of this policy also allows private citizens to file civil lawsuits against abortion providers or individuals who assist someone in obtaining an abortion, including through transportation or financial support³.
While abortion care is widely recognized as one of the safest medical procedures when performed legally and under appropriate medical supervision⁴, legal restrictions continue to limit access to safe reproductive healthcare. And debates surrounding these policies often center on fundamental human rights, including bodily autonomy, privacy, equality, and access to healthcare.
The diagrams below were designed to make systemic relationships visible. Maternal mortality is often discussed through isolated statistics, but visual mapping reveals how healthcare access, policy restrictions, economic instability, and racial inequities operate as interconnected systems rather than separate issues. Organizing these factors visually helps expose patterns that are otherwise difficult to identify through data alone.
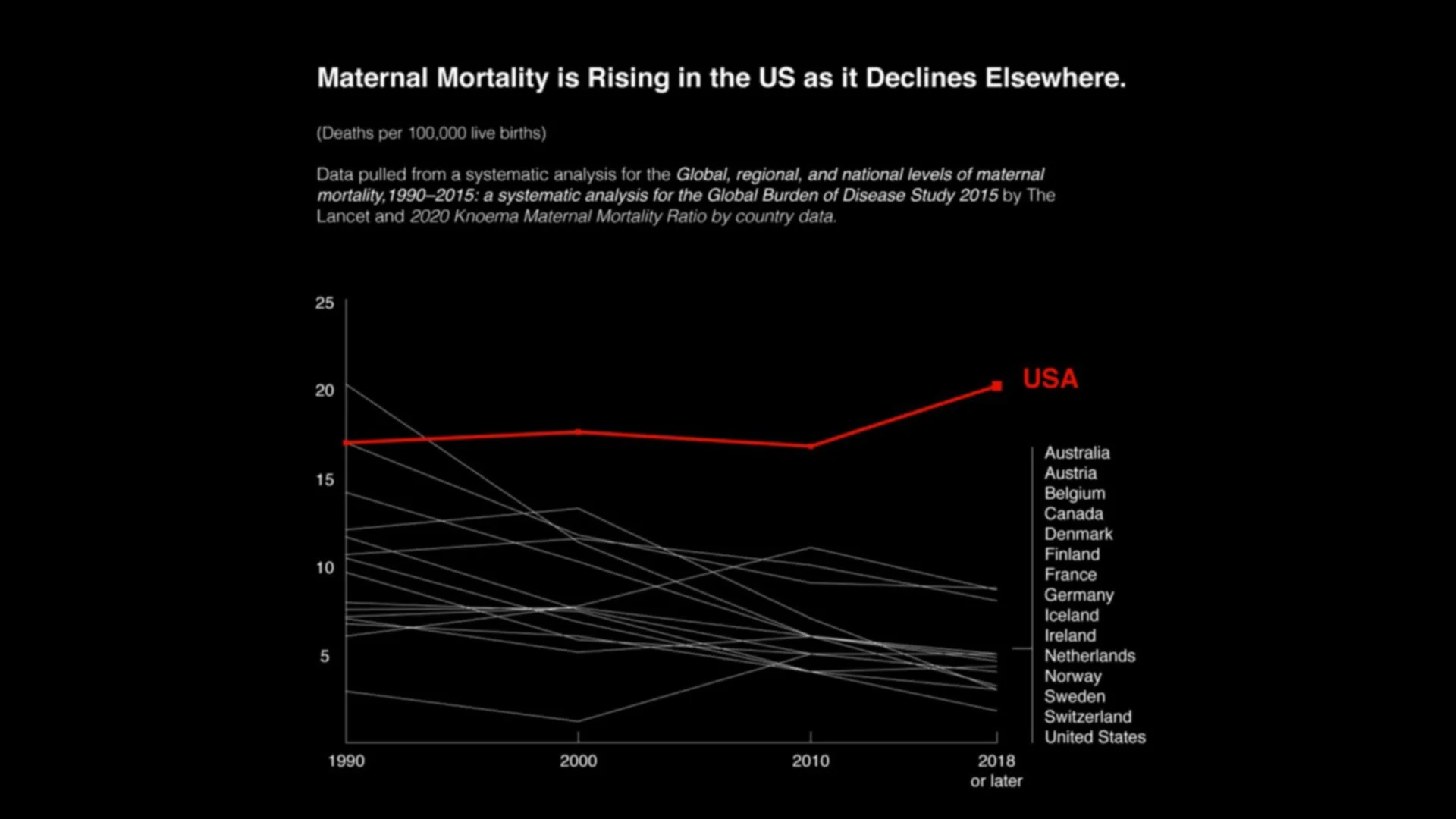
Data sources: The Lancet and Knoema
The COVID-19 pandemic intensified existing weaknesses within the U.S. healthcare system. Research indicates that the first 18 months of the pandemic saw increases in maternal mortality and stillbirths, particularly among women in low-resource communities and among Black women in the United States⁵. During this same period, Texas introduced additional restrictions on abortion procedures, citing the need to conserve medical resources during the pandemic⁶. As a result, many residents were forced to travel out of state to obtain care.
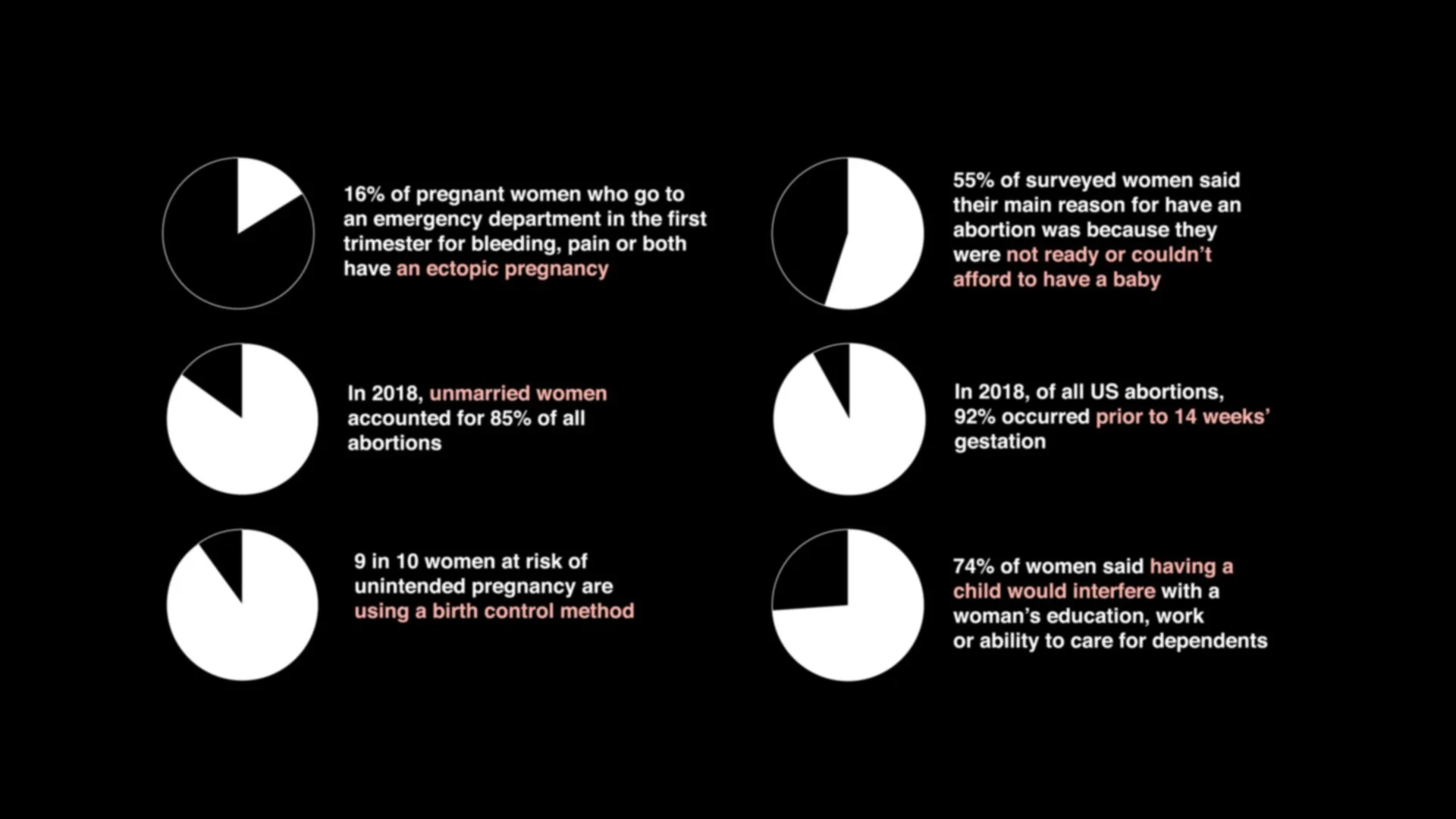
Additionally, public debate surrounding abortion often overlooks the complexity of reproductive decision-making. Research conducted by the Guttmacher Institute found that the most frequently reported reasons for seeking an abortion include financial instability, the potential impact of pregnancy on existing children or family responsibilities, and concerns surrounding relationships or single parenthood⁷. Health considerations affecting either the fetus or the pregnant individual are also commonly cited.
Understanding these realities is essential for developing policies that support maternal health rather than restrict access to care.
The well-being of mothers and infants should remain a core public health priority. Effective maternal healthcare depends not only on medical access, but on the design of the systems surrounding care itself.
Families must be able to navigate prenatal appointments, insurance policies, postpartum recovery resources, transportation, childcare, and emergency support networks — all of which rely on clear communication, accessible information, and coordinated service design.
Many pregnancy-related complications occur months after delivery, yet healthcare coverage and support frequently end shortly after birth.
Closing these gaps requires coordinated care networks supported by accessible communication systems that help mothers understand what services exist, when support is needed, and how to access care before complications escalate. In practice, this is also a design problem: information that is fragmented, inaccessible, or difficult to navigate can directly impact health outcomes.
Community-led organizations often step in where formal systems fall short, connecting families with education, advocacy, and postpartum support. Sustaining and expanding these efforts depends on consistent funding and policy support, as they play an important role in strengthening maternal health infrastructure and improving outcomes for mothers and infants.
This project ultimately became an exercise in impact communication and systems visualization. Maternal mortality is frequently framed as an individual medical issue, when in reality it reflects the cumulative effects of policy decisions, economic inequality, healthcare infrastructure, and information accessibility. Design plays a role in how these systems are understood. When research, data, and lived realities are organized clearly, patterns become more visible. This matters because it makes systemic failures become harder to ignore.
Selected Research and References:
¹ Commonwealth Fund. Maternal Mortality and Maternity Care in the United States Compared to 10 Other Developed Countries. Published November 2020.
² The New York Times. Texas’s Near-Total Abortion Ban Takes Effect After Supreme Court Inaction. Published September 2021.
³ The Guardian. Texas Now Has Abortion “Bounty Hunters”: Read Sonia Sotomayor’s Scathing Legal Dissent. Published September 2021.
⁴ World Health Organization (WHO). WHO Issues New Guidelines on Abortion to Help Countries Deliver Lifesaving Care. Published March 2022.
⁵ BMJ Global Health. COVID-19 and Maternal and Perinatal Outcomes. Published August 2021.
⁶ Office of the Texas Governor. Governor Abbott Issues Executive Order Increasing Hospital Capacity, Announces Supply Chain Strike Force for COVID-19 Response. Published March 2020.
⁷ Guttmacher Institute. Reasons U.S. Women Have Abortions: Quantitative and Qualitative Perspectives. Published September 2005.